
Autoarterial revascularization of myocardium involving Y-composite grafts and in situ conduits of the internal thoracic arteries: randomized controlled trial, hospital and mid-term outcomes
 A.K. Sabetov
A.K. Sabetov- D.A. Sirota
- D.S. Khvan
- M.O. Zhulkov
- A.A. Shadanov
- A.M. Chernyavskiy
Published 2024-08-30
Keywords
- Coronary Artery Bypass,
- Coronary Artery Disease,
- Follow-Up Studies,
- Mammary Arteries,
- Myocardium
How to Cite
Copyright (c) 2024 Sabetov A.K., Sirota D.A., Khvan D.S., Zhulkov M.O., Shadanov A.A., Chernyavskiy A.M.

This work is licensed under a Creative Commons Attribution 4.0 International License.
Abstract
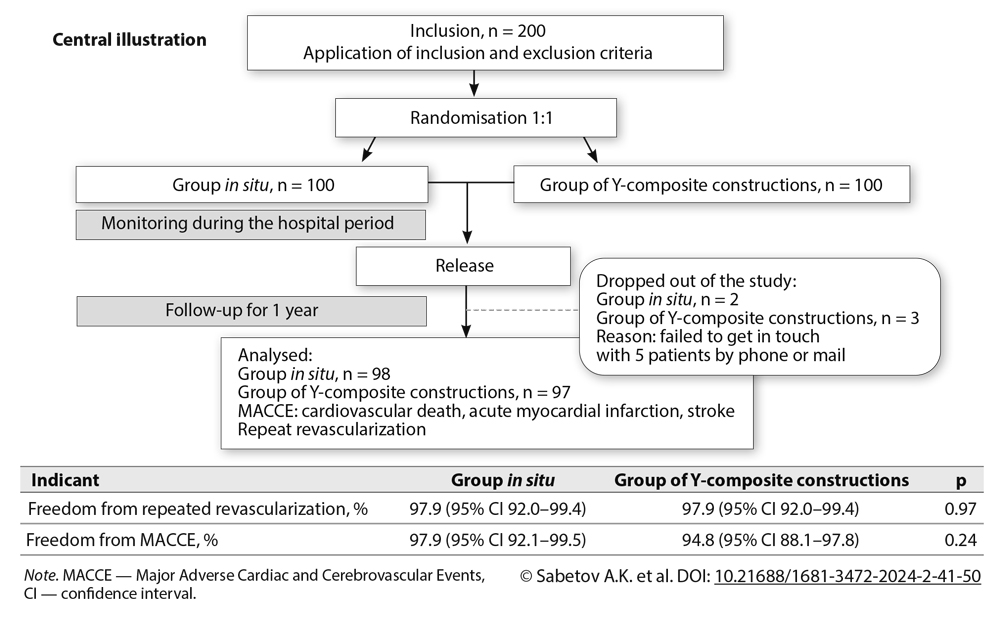
Objective: The aim of this study was to evaluate the outcomes of autoarterial revascularization involving Y-composite grafts and in situ conduits out of the internal thoracic arteries (ITAs) at the hospital period and after a year follow-up.
Methods: The study included 200 patients with coronary artery disease who underwent coronary bypass surgery over the period from March 2018 to March 2021. Patients were randomized using the envelope method into 2 groups: in the first group, autoarterial conduits out of the ITAs were used according to the in situ method (n = 100); in the second group, autoarterial conduits with the formation of a Y-composite grafts out of ITAs (n = 100) were put into practice. The primary endpoints of the study were the incidence of repeat revascularization and amount of major adverse cardiac and cerebrovascular events (MACCE).
Results: There was no significant difference between the two groups in the level of freedom from MACCE; in the in situ and Y-composite groups the indicators were 97.9% (95% CI 92.1-99.5) and 94.8% (95% CI 88.1‑97.8; P = 0.24), respectively. In a year follow-up, freedom from repeated revascularization amounted to 97.9% in the in situ group (95% CI 92-99.4), and 97.9% in the Y-composite group (95% CI 91.9-99.4; P = 0.97). A significant difference was registered in the surgery duration, which in the in situ group lasted 235 [197.5; 252.5] minutes versus 252.5 [225; 290] minutes in the Y-composite group, P < 0.002. In the Y-composite group, the rate of infectious complications on the breast bone was significantly more frequent than in the in situ group (P < 0.023).
Conclusion: Despite the hypothetical advantages of bimammar coronary bypass surgery over the Y-configuration one, this study did not reveal significant differences in outcomes between the in situ and Y-composite groups.
Received 7 November 2023. Revised 10 June 2024. Accepted 24 June 2024.
Funding
The study did not have sponsorship.
Conflict of interest
The authors declare no conflict of interest.
Contribution of the authors
Conception and study design: A.K. Sabetov, D.S. Khvan, M.O. Zhulkov
Data collection and analysis: A.K. Sabetov
Statistical analysis: A.A. Shadanov, A.K. Sabetov
Drafting the article: A.K. Sabetov
Critical revision of the article: D.A. Sirota, D.S. Khvan, A.M. Chernyavskiy
Final approval of the version to be published: A.K. Sabetov, D.A. Sirota, D.S. Khvan, M.O. Zhulkov, A.A. Shadanov, A.M. Chernyavskiy
References
- Жбанов И.В., Мартиросян А.К., Урюжников В.В., Киладзе И.З., Галимов Н.М., Ревишвили Г.А., Шабалкин Б.В. Множественное коронарное шунтирование с использованием двух внутренних грудных артерий. Клин. и эксперимент. хир. Журн. им. акад. Б.В. Петровского. 2018;6(4):66-74. https://doi.org/10.24411/2308-1198-2018-14010 Zhbanov I.V., Martirosyan A.K., Uryuzhnikov V.V., Kiladze I.Z., Galimov N.M., Revishvili G.A., Shabalkin B.V. Multiple coronary artery bypass surgery using two internal thoracic arteries. Clin Experiment Surg. Petrovsky J. 2018;6(4):66-74. (In Russ.) https://doi.org/10.24411/2308-1198-2018-14010
- Yusuf S., Zucker D., Peduzzi P., Fisher L.D., Takaro T., Kennedy J.W., Davis K., Killip T., Passamani E., Norris R., Morris C., Mathur V., Varnauskas E., Chalmers T.C. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet. 1994;344(8922):563-570. PMID: 7914958. https://doi.org/10.1016/s0140-6736(94)91963-1
- Taggart D.P. Thomas B. Ferguson Lecture. Coronary artery bypass grafting is still the best treatment for multivessel and left main disease, but patients need to know. Ann Thorac Surg. 2006;82(6):1966-1975. PMID: 17126093. https://doi.org/10.1016/j.athoracsur.2006.06.035
- Glineur D., Hanet C., Poncelet A., D'hoore W., Funken J.C., Rubay J., Kefer J., Astarci P., Lacroix V., Verhelst R., Etienne P.Y., Noirhomme P., El Khoury G. Comparison of bilateral internal thoracic artery revascularization using in situ or Y graft configurations: a prospective randomized clinical, functional, and angiographic midterm evaluation. Circulation. 2008;118(14 Suppl):S216-221. PMID: 18824757. https://doi.org/10.1161/CIRCULATIONAHA.107.751933
- Hwang H.Y., Oh H.C., Kim Y.H., Kim K.B. Complete revascularization of the three vessel territories using a left internal thoracic artery composite graft. Ann Thorac Surg. 2015;100(1):59-66. https://doi.org/10.1016/j.athoracsur.2015.01.068
- Otsuka F., Yahagi K., Sakakura K., Virmani R. Why is the mammary artery so special and what protects it from atherosclerosis? Ann Cardiothorac Surg. 2013;2(4):519-526. https://doi.org/10.3978/j.issn.2225-319X.2013.07.06
- Lytle B.W., Blackstone E.H., Loop F.D., Houghtaling P.L., Arnold J.H., Akhrass R., McCarthy P.M., Cosgrove D.M. Two internal thoracic artery grafts are better than one. J Thorac Cardiovasc Surg. 1999;117(5):855-872. PMID: 10220677. https://doi.org/10.1016/S0022-5223(99)70365-X
- Neumann F.J., Sousa-Uva M., Ahlsson A., Alfonso F., Banning A.P., Benedetto U., Byrne R.A., Collet J.P., Falk V., Head S.J., Jüni P., Kastrati A., Koller A., Kristensen S.D., Niebauer J., Richter D.J., Seferovic P.M., Sibbing D., Stefanini G.G., Windecker S., Yadav R., Zembala M.O.; ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87-165. PMID: 30165437. https://doi.org/10.1093/eurheartj/ehy394
- Акчурин Р.С., Ширяев А.А., Васильев В.П., Галяутдинов Д.М., Власова Э.Е. Современные тенденции в коронарной хирургии. Патология кровообращения и кардиохирургия. 2017;21(3S):34-44. https://doi.org/10.21688/1681-3472-2017-3S-34-44 Akchurin R.S., Shiryaev A.A., Vasiliev V.P., Galyautdinov D.M., Vlasova E.E. Modern trends in coronary surgery. Patologiya krovoobrashcheniya i kardiokhirurgiya = Circulation Pathology and Cardiac Surgery. 2017;21(3S):34-44. (In Russ.). https://doi.org/10.21688/1681-3472-2017-3S-34-44
- Gaudino M., Taggart D., Suma H., Puskas J.D., Crea F., Massetti M. The choice of conduits in coronary artery bypass surgery. J Am Coll Cardiol. 2015;66(15):1729-1737. PMID: 26449144. https://dx.doi.org/10.1016/j.jacc.2015.08.395
- Lytle B.W., Cosgrove D.M., Saltus G.L., Taylor P.C., Loop F.D. Multivessel coronary revascularization without saphenous vein: long-term results of bilateral internal mammary artery grafting. Ann Thorac Surg. 1983;36(5):540-547. PMID: 6639193. https://doi.org/10.1016/s0003-4975(10)60684-4
- Sauvage L.R., Wu H.D., Kowalsky T.E., Davis C.C., Smith J.C., Rittenhouse E.A., Hall D.G., Mansfield P.B., Mathisen S.R., Usui Y., Goff S.G. Healing basis and surgical techniques for complete revascularization of the left ventricle using only the internal mammary arteries. Ann Thorac Surg. 1986;42(4):449-465. PMID: 3490233. https://doi.org/10.1016/s0003-4975(10)60557-7
- Kawajiri H., Grau J.B., Fortier J.H., Glineur D. Bilateral internal thoracic artery grafting in situ or composite? Ann Cardiothorac Surg. 2018;7(5):673-680. PMID: 30505752; PMCID: PMC6219951. https://doi.org/10.21037/acs.2018.05.16
- Gatti G., Castaldi G., Morosin M., Tavcar I., Belgrano M., Benussi B., Sinagra G., Pappalardo A. Double versus single source left-sided coronary revascularization using bilateral internal thoracic artery graft alone. Heart Vessels. 2018;33(2):113-125. PMID: 28801799. https://doi.org/10.1007/s00380-017-1040-1
- Сабетов А.К., Сирота Д.А., Хван Д.С., Жульков М.О., Чернявский А.М. Артериальная реваскуляризация миокарда с использованием Y-композитных конструкций и in situ кондуитов внутренних грудных артерий: непосредственные результаты. Патология кровообращения и кардиохирургия. 2020;24(4):63-71. https://doi.org/10.21688/1681-3472-2020-4-63-71 Sabetov A.K., Sirota D.A., Khvan D.S., Zhulkov M.O., Chernyavskiy A.M. Arterial revascularisation using in situ or Y-composite conduits of internal thoracic arteries: Early results. Patologiya krovoobrashcheniya i kardiokhirurgiya = Circulation Pathology and Cardiac Surgery. 2020;24(4):63-71. (In Russ.) https://doi.org/10.21688/1681-3472-2020-4-63-71
- Glineur D., Boodhwani M., Hanet C., de Kerchove L., Navarra E., Astarci P., Noirhomme P., El Khoury G. Bilateral internal thoracic artery configuration for coronary artery bypass surgery: a prospective randomized trial. Circ Cardiovasc Interv. 2016;9(7):e003518. PMID: 27406988. https://doi.org/10.1161/CIRCINTERVENTIONS.115.003518
- Lev-Ran O., Paz Y., Pevni D., Kramer A., Shapira I., Locker C., Mohr R. Bilateral internal thoracic artery grafting: midterm results of composite versus in situ crossover graft. Ann Thorac Surg. 2002;74(3):704-711. PMID: 12238828. https://doi.org/10.1016/s0003-4975(02)03791-8
- Ogawa S., Tsunekawa T., Hosoba S., Goto Y., Kato T., Kitamura H., Tomita S., Okawa Y. Bilateral internal thoracic artery grafting: propensity analysis of the left internal thoracic artery versus the right internal thoracic artery as a bypass graft to the left anterior descending artery. Eur J Cardiothorac Surg. 2020;57(4):701-708. PMID: 31638700. https://doi.org/10.1093/ejcts/ezz290
- Magruder J.T., Young A., Grimm J.C., Conte J.V., Shah A.S., Mandal K., Sciortino C.M., Zehr K.J., Cameron D.E., Price J. Bilateral internal thoracic artery grafting: Does graft configuration affect outcome? J Thorac Cardiovasc Surg. 2016;152(1):120-127. PMID: 27343909. https://doi.org/10.1016/j.jtcvs.2016.03.022